
Did you know that the ancient Greeks had a word for celiac disease? Or that research indicates gluten might not be the only culprit for millions of people with gluten sensitivity? Or that treatments beyond a gluten-free diet might be on the horizon?
In March, I co-presented a talk with John Gildae, PhD, at Natural Products Expo West 2015 on The Evolution of Gluten and Gut Health. My part covered the history, current state, and future projections of celiac disease and the gluten-free movement. Dr. John followed up with a science-based look at how gluten affects the gut, current statistics regarding its effect, and in-the-works treatments for those with celiac disease and gluten sensitivity. (For more about his work, contact him at johnjgildae@gmail.com.)
Several people have asked me for a review of that talk, so here it is, along with my slides.
Please keep in mind: I am not a scientist or a health care professional. I presented my material from a journalist’s perspective and that of a mom: My son, Sam, became severely gluten intolerant while at college after showing absolutely no signs of gluten intolerance while growing up. Today, both he and my daughter eat a strictly gluten-free diet.
I gleaned much of my information from the excellent book Gluten Freedom by Alessio Fasano, MD, whom many consider to be the foremost authority on celiac disease and gluten sensitivity.

Slide 1: Celiac disease’s early history
Wheat, and by extension the gluten protein that’s also found in rye and barley, has been part of human evolution for 10,000 years, since the dawn of farming. About 2,000 years ago, a Greek physician named Aretaeus coined the term koiliakos (for “suffering in the bowels”), the word that eventually became “celiac.”
But not until the 1880s did celiac disease appear in the medical literature. At that time, a British physician, Dr. Samuel Gee, gave a talk that established the first medical definition of celiac disease (CD) as a malabsorption triggered by some kind of food. In his words, CD was “a kind of chronic indigestion which is met in persons of all ages, yet … especially apt to affect children between 1 and 5 years old.”
Dr. Gee was right on target when he said that “if a patient can be cured at all, it must be by means of diet.” Unfortunately, his treatment consisted of thinly cut and well-toasted bread. (Fail.)
Then, in the 1920s, a New York City pediatrician named Dr. Sidney Haas developed the banana diet for celiac disease, giving rise to an entire generation of children called banana babies. The diet worked—there’s no gluten in bananas, after all—but again missed the mark for causation. Even so, the banana diet remained the standard therapy for another 30-40 years.
Then came a true breakthrough: In the 1940s-50s, Dr. Willem-Karel Dicke of the Netherlands definitively connected gluten as the dietary trigger for CD, thus giving rise to the first effective and lasting treatment: the gluten-free diet. (Consequently, Dicke is rightly considered the father of the gluten-free diet.) At this time CD was thought to be a gastrointestinal condition confined to northern Europe and Caucasians, and, still, primarily children.
In the 1960s-70s, improved diagnostic tools made it possible to see actual CD biomarkers: flattened intestinal villi, which became the defining hallmark of CD. Rather than healthy fingerlike projections, as seen in Slide 1, CD-damaged villi look like the top of a marshmallow. This biomarker also helped distinguish CD from a food allergy, which is a histamine-based and anaphylactic response that the body can outgrow. In contrast, CD was now classified as an autoimmune condition, which one does not outgrow. If you have CD, you have it for life, though the intestinal tissue damage can, in fact, be reversed.
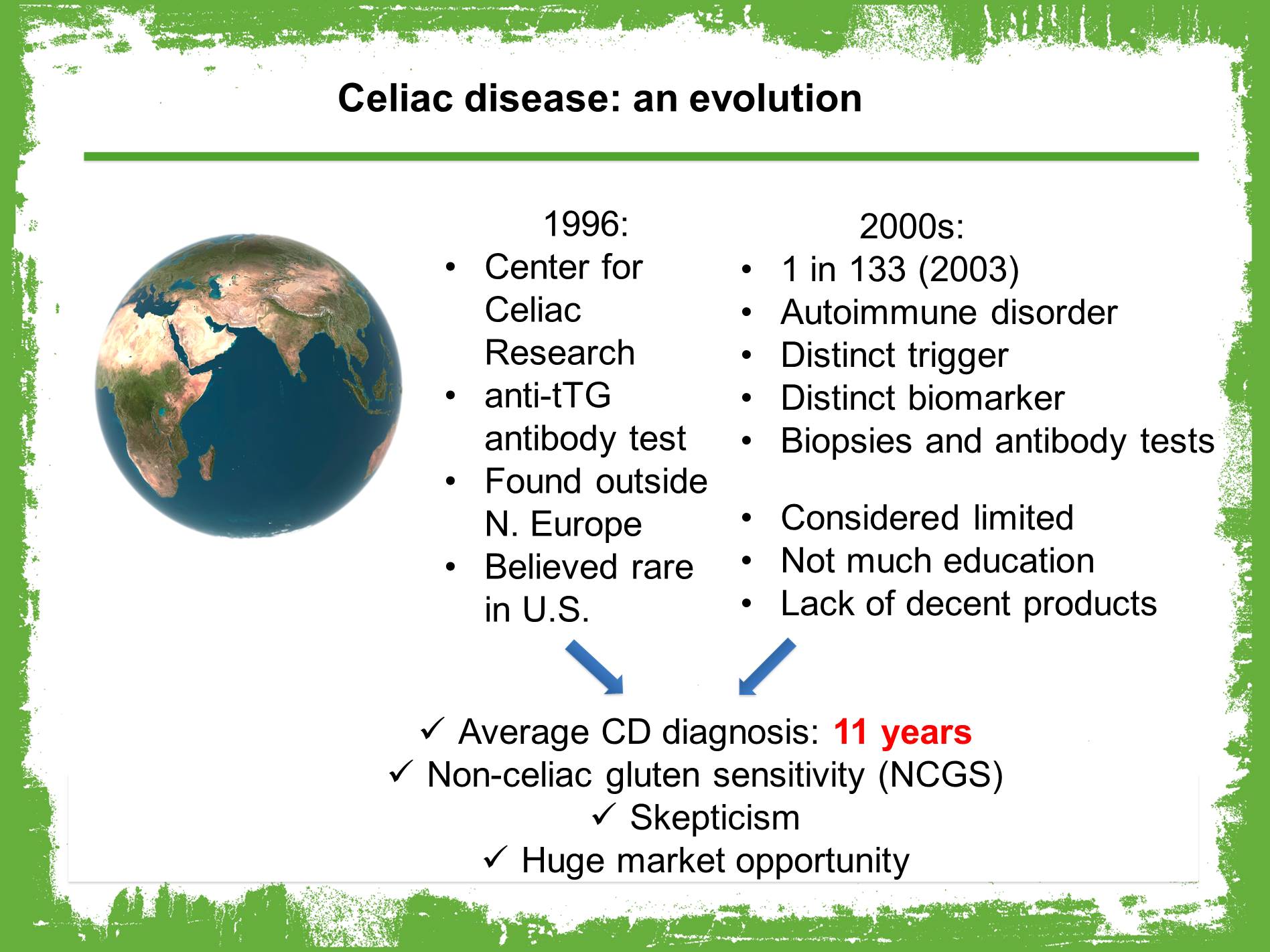
Slide 2: CD evolution, 1996-2000s
In 1996—amazingly, less than 20 years ago—the Center for Celiac Research (CCR) was established in Maryland (now at Mass General) as the first CD, wheat allergy, and gluten sensitivity research and treatment center in the U.S.
At that time, CD numbers worldwide were thought to be 1 in 184 – and it was discovered not just in Europe, but also in Libya, Egypt, north Africa, India and China. CD was, however, still considered rare to nonexistent in the U.S.
The CCR also undertook a 5-year study of celiac disease incidence, and also developed the anti-tTG antibody test now used worldwide to diagnose CD, which greatly reduced the need for repeat biopsies.
In summary, here’s what was understood about CD at that time:
- It’s real; a landmark 2003 report in the Archives of Internal Medicine put the incidence of CD at 1 in 133
- It’s an autoimmune condition, where the body attacks itself in response to a trigger
- It has a distinct trigger: gluten
- It has a distinct biomarker: flattened villi
- Biopsies and antibody tests can accurately diagnose
Furthermore:
- CD was though to be limited geographically and in frequency
- There was still not much education about it, for health care professionals or consumers
- There was a real lack of decent GF products. Early attempts were, by all accounts, terrible: crumbly, cardboard-like, and not nutritious, made with extra sugar, salt, and fat plus empty-calorie staples like white rice flour and potato starch to make up for the lack of good texture and taste. Still, people with CD were happy to have anything…
Consequently, in the late 1990s and early 2000s:
- The average length of time to diagnosis CD was 11 years. Think about that for a second. That’s an awfully long time to have doctors puzzled or telling you your illness is all in your head.
- The 1 in 133 study led people to go to doctors to check for CD; however, when CD was ruled out, most physicians simply told people that wheat and gluten were not the problem. Nevertheless, more people started eliminating gluten … and felt better. This led to the concept of non-celiac gluten sensitivity (NCGS), which was finally established in 2010 as a distinct medical condition from CD, though without biomarkers.
- There was a lot of skepticism about both CD and NCGS
- There was a huge market opportunity for great GF products
Slide 3: CD evolution, 2000
The year 2000 also saw two more major milestones:
- the mapping of the human genome and the new possibility of personalized medicine
- the CCR’s discovery of zonulin, a human protein that modulates gut permeability. According to the CCR, too much zonulin causes increased gut permeability in CD and is also linked to many other autoimmune diseases, including type 1 diabetes, multiple sclerosis, and rheumatoid arthritis.

Slide 4: Why are so many people eating gluten free?
Let’s take a slight detour into the manufacturing scene. As many people know, sales of GF foods exploded in the past 5-8 years, going from $4 billion in 2007 to just over $8 billion in 2012, with a projection of $18 billion by 2018 (Nutrition Business Journal Special Diets report).
This growth can’t be explained by people with CD disease alone (even though the rate of CD is doubling every 15 years; see link under Slide 7).
This gives rise to the question: Why are so many people buying and eating GF foods?
- Better education and awareness of CD. At long last, celiac disease and gluten sensitivity are mainstream topics. In addition, families and friends of people who need to eat gluten free get on board with the GF diet, leading to increased sales.
- Better quality! Several natural foods pioneers, characteristically ahead of the curve, took the helm to create truly good-tasting GF foods (for example, Glutino in 1983, Bob’s Red Mill around 1985, and Pamela’s Products in 1988). In the mid-2000s, innovators began to up the ante with whole-food, nutrient-rich ingredients like brown rice, nut flours, quinoa, flaxseed, chia, coconut, and more (for example, Purely Elizabeth and Hail Merry). Today’s GF foods rival their glutinous counterparts for taste and, increasingly, nutrition. Anyone who thinks otherwise hasn’t been paying attention.
- Increased consumer confidence in safe, packaged gluten-free foods. This was a long time coming and remains an important education component for both manufacturers and consumers. The first major step forward was the 2004 Food Allergen Labeling and Consumer Protection Act (FALCPA), which mandated disclosure of the top eight most common food allergens, including wheat, on all food labels. However, this did not cover non-wheat foods, such as barley, that contain gluten, so trustworthy third-party certifications stepped into the gap. Finally, the FDA’s long-awaited standard for labeling a food as gluten free went into effect in August 2014. Also, manufacturers of naturally GF foods are now labeling them as such, further reducing consumers’ confusion about whether a food is “safe.”
- Then there’s the matter of food tribes, fads, alarms, and impressions, all of which contribute to GF sales.
- 30% of US adults minimize or eliminate gluten. That’s an astonishing number! Lessertarians and Ancientarians fall into this category: paleo eaters who eschew all grains (therefore eliminating gluten), and people returning to heirloom or ancient grains, many of which are naturally gluten free or of a less-processed wheat variety, like Kamut. Old-school bread making, which encourages fermentation, is also enjoying a comeback, with some sourdough evangelists insisting that slowly fermented bread exerts a much less detrimental impact on the gut than quick-processed modern bread. Many people simply have a vague idea that eating less gluten is generally healthier — and with so many good-tasting options now available, why not?
- Celebrity endorsements and especially weight loss are huge draws. One-fourth of GF eaters are doing it for weight loss. This is misguided. If you’re eating GF, you do tend to lower intake of all refined carbohydrates, which can trim pounds in the short run; but nutrition experts agree that it is most definitely not a weight loss diet.
- Alarms about gluten being a poison for everyone (the Wheat Belly and Grain Brain camps) cause some people to give it up or reduce it in their diets.
- A sense that “if it’s good for you, it might be good for me” leads people to try eliminating gluten. This wouldn’t necessarily translate to more long-term gluten-free eaters … except for the fact that many people do feel better and therefore keep at it.
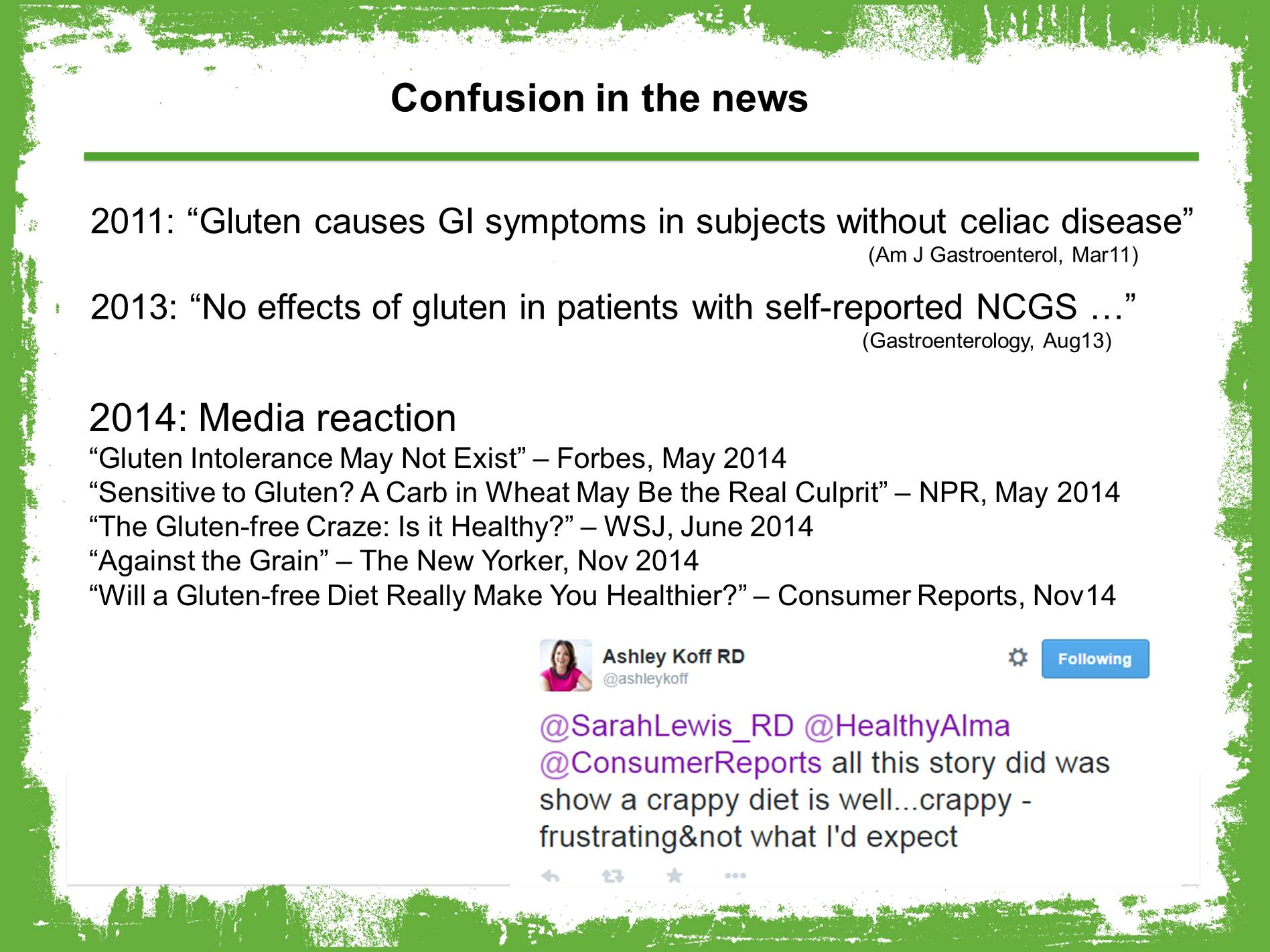
Slide 5: Confusion in the news
Unfortunately, the fad mentality creates a confusing environment that media is all too happy to misreport.
In 2011, an Australian research group published a double-blind, placebo-controlled study that supported the evidence that non-celiac gluten sensitivity is real.
But then, in 2013, the same study authors published a follow-up that seemed to contradict their original study: “in contrast to our first study, we could find absolutely no specific response to gluten.”
The suspected culprit: FODMAP foods, highly fermentable but poorly absorbed carbohydrates. (More on this in a minute.)
In 2014, the media world exploded with relish:
- “Gluten Intolerance May Not Exist” (Forbes, May 2014)
- “Sensitive to Gluten? A Carb in Wheat May Be the Real Culprit” (NPR, May 2014)
- “The Gluten-Free Craze: Is it Healthy?” (Wall St. Journal, June 2014) [Note the use of the word “craze.”]
- “Against the Grain” (The New Yorker, Nov 2014)
- “Will a Gluten-Free Diet Really Make You Healthier?” (Consumer Reports, Nov 2014)
The Consumer Reports article in particular was surprisingly out of touch; it compared early-generation, empty-calorie and nutrient-devoid GF muffins with “regular” muffins for sugar, fiber, and such, while completely ignoring the wealth of delicious and nutrient-dense options now available to GF eaters. I appreciated Ashley Koff’s tweet after the CR story came out: “All this story did was show that a crappy diet is well…crappy – frustrating & not what I’d expect.” Amen, sister!
Slide 6: Is it gluten, or something else?
The real takeaway from that second, “contradictory” study was the focus on FODMAP foods. FODMAP stands for Fermentable, Oligo, Di-, Mono-saccharides And Polyols — carbohydrates (sugars), found in a wide variety of foods, that are poorly digested or absorbed, which can lead to digestive distress.
Researchers found that reintroducing gluten didn’t necessarily cause a reaction in subjects, but FODMAP foods did. In other words, a carb in wheat might be causing the very real symptoms now attributed to gluten.
In February, I came across a brand-new food label that’s already on some packaged foods in Australia: FODMAP Friendly. I’m now wondering whether we’ll start seeing this new label on foods here in the U.S. soon.
In light of the media firestorm and resultant confusion, I appreciated and recommend Jennifer Iscol’s May 2014 article, “Fake Gluten Sensitivity or Incendiary Journalism.” In it, she quotes Amy Burkhart, MD, RD: “Perhaps gluten sensitivity will soon be given a new name as it doesn’t appear the gluten is always the issue.”
Might we start hearing “wheat sensitivity”? Perhaps even “FODMAP sensitive”?
Keep in mind, as Dr. Burkhart points out: “The existence of celiac disease is not under debate. It is non-celiac gluten sensitivity that is under the microscope.”
Slide 7: Current estimates of CD and NCGS
With celiac disease and gluten research continuing, here’s where we stand today. According to current reliable estimates:
- Up to 3 million (1%) people in the U.S. have CD. That number marks CD as humankind’s most prevalent genetically linked disease and, experts believe, represents the tip of the iceberg.
- Currently time of diagnosis averages 4 years — certainly better than 11 years, but still a tough slog for people who are suffering with this condition. It’s also compelling evidence that consumer and health care education remains crucial.
- Only a fraction (<200K) of those 3 million people are diagnosed. In developed countries, experts estimate that there are 5-10 undiagnosed CD cases for every 1 case diagnosed.
- 20 million (6%) fall on the spectrum of NCGS
- 900,000 (0.1-0.4%) have a wheat allergy (anaphylactic)
As mentioned earlier, a 2010 study of 3,000 healthy adults for 50 years found that the rate of CD is doubling every 15 years, “due to an increasing number of subjects that lost the immunological tolerance to gluten in their adulthood,” according to study authors.
“Something has changed in our environment that’s driving an increased incidence of celiac disease,” said Joseph Murray, MD, a Mayo Clinic gastroenterologist, in a March 2013 Reuters article. “Whatever has happened with CD has happened since 1950; the increase affected young and old people equally,” he added in a 2014 article.
Slide 8: Why the change from gluten tolerance to intolerance?
So, the big question that I get asked all the time: WHY has the human body switched from gluten tolerance to CD and gluten sensitivity? After all, people ate gluten safely for thousands and thousands of years; as a friend asked me skeptically just last month, “why the hell is gluten suddenly such a problem?” What has happened to make CD and NCGS so prevalent and, indeed, increasing?
Many theories exist. Among them:
- In developed countries, some grains are bred for higher gluten content to make them more hearty for industrial processing methods. (This is not to be confused with genetically modified organisms, or GMOs; no GMO wheat is currently allowed anywhere in the world.) And gluten isn’t confined to typical foods like bread anymore; in the past few decades its concentrated form, especially vital wheat gluten, has been added to innumerable packaged, processed foods. So the typical person is inadvertently ingesting a lot more gluten on a daily basis than our ancestors did.
- The hygiene theory, which posits that our modern love of antibacterial soaps and cleanliness has actually negatively affected the human immune system
- Overuse and abuse of antibiotics, which again thrashes the immune system and disrupts a healthy human microbiome
- Overreliance on baby formula and C-sections, which prevent normal, healthy bacteria in breast milk and the vaginal canal from becoming established in infants
- Environmental impacts: glyphosates (our friendly neighborhood RoundUp) applied to GMO crops that negatively affect the intestinal tight junctions
Incidentally, addressing gut permeability may hold the best promise for effective therapies beyond lifelong adherence to a gluten-free diet. In a 2012 research study, Dr. Fasano wrote, “The classical paradigm of autoimmune [disease arising from] gene makeup and exposure to environmental triggers has been recently challenged by the addition of a third element, the loss of intestinal barrier function [i.e., the breakdown of tight junctions]. … New therapeutic strategies aimed at reestablishing the intestinal barrier function offer innovative, unexplored approaches for the treatment of these devastating diseases.”
According to another 2012 study, non-GF-diet treatments currently being explored include zonulin-blockage therapies, a therapeutic vaccine to induce gluten tolerance, and degrading the gluten protein using probiotics.
Slide 9: the microbiome connection
Researchers are now really focusing on how one or a combination of these and other theoretical causes are affecting the human microbiome and therefore gut health in general. As Dr. Fasano says in Gluten Freedom, “What happens to [people] to make them switch from tolerance to the immune response that leads to celiac disease? I believe the answer … is indeed related to changes in the microbiome.”
(For an excellent overview of the microbiome, I recommend this short NPR video, The Invisible Universe of the Human Microbiome.)
Is gluten-free here to stay? Absolutely. Celiac disease is real and on the rise; gluten sensitivity, whether from wheat or FODMAPs or changes in gut bacteria, is also real and on the rise. As stated in a December 2014 report by the Hartman Group, “The lasting growth [in gluten-free purchasing and eating] rests with people who avoid gluten in order to improve their digestion, and who do it by eating less processed, whole-grain foods. … Gluten free reflects the cultural belief that digestion is the root of all wellness.”

Pingback: Kitul nectar: a new (old) organic sweetener |
Pingback: 3 surprising reasons to love the paleo diet |
Pingback: 5 tips to choose a wedding menu |